
byJustin Jackson, Medical Xpress
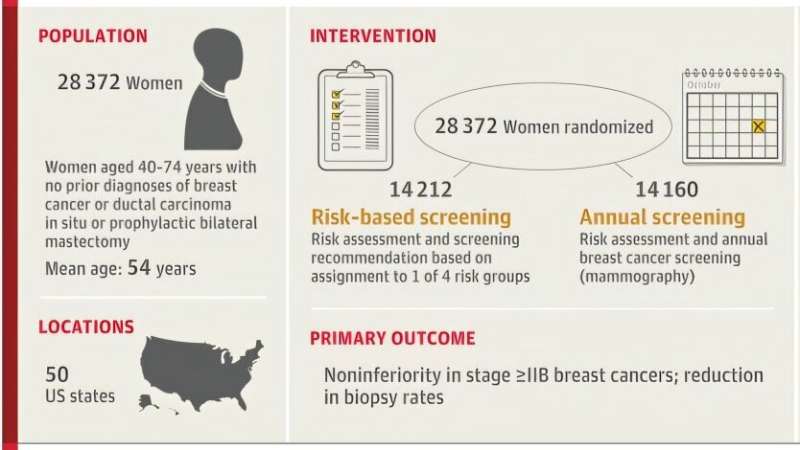
Visual abstract. Credit:JAMA(2025). DOI: 10.1001/jama.2025.24784
University of California, San Francisco investigators led WISDOM, a randomized comparison of risk-based breast cancer screening and annual mammography. Rates of stage ≥IIB breast cancers met a noninferiority threshold under risk-based screening, and breast biopsy rates ran higher rather than lower.
Age-based screening treats breast cancer risk as broadly similar across women of the same age range. Previous work has shown wide variation in risk tied to factors such as breast density, single-nucleotide gene variants combined.
Population-based screening has been associated with more stage I disease diagnoses without a matching drop in later-stage disease, more in situ lesions without an equivalent drop in early-stage invasive cancers, symptomatic or interval cancers between periodic screens, high false-positive rates with many benign biopsies, and high resource demands tied to screening costs. If broad screening is not having a positive effect on outcomes, another strategy may be needed.
In the study, "Risk-Based vs. Annual Breast Cancer Screening," published inJAMA, researchers conducted a pragmatic randomized trial to determine whether risk-based screening can serve as an alternative to annual mammography.
Researchers randomized 28,372 women aged 40 to 74 years with no prior breast cancer or ductal carcinoma in situ and no prophylactic bilateral mastectomy. Risk assessment combined sequencing ofnine susceptibility genes, a polygenic risk score, and the Breast Cancer Surveillance Consortium version 2 model.
Risk-based recommendations used four categories. Highest risk reflected a 6% five-year risk or ahigh-penetrance pathogenic variant, paired with alternating mammography and magnetic resonance imaging every six months and counseling.
Elevated risk reflected the top 2.5% risk percentile by age, paired with annual mammography and risk-reduction counseling.Average riskreflected women aged 50 years with risk below 6% and below the top 2.5th percentile by age, paired with biennial mammography. The lowest risk reflected women aged 40 to 49 years with a five-year risk under 1.3%, paired with no screening until risk reached 1.3% or greater or age 50 years.
Coprimary outcomes paired safety and morbidity. Stage ≥IIB breast cancers served as the noninferiority end point, and biopsy rates served as the end point for superiority testing in reducing biopsies.
Stage ≥IIB breast cancers occurred less often in the risk-based group than in the annual group, with 21 vs. 31 events and rates of 30.0 vs. 48.0 per 100,000 person-years, yielding a rate difference of −18.0 per 100,000 person-years.
Breast biopsy rates were higher in the risk-based group, with a reported rate difference of 98.7 per 100,000 person-years. Mammogram use ran lower in the risk-based group, with a reported rate difference of −3,835.9 per 100,000 person-years. Magnetic resonance imaging use was higher in the risk-based group, with highest and elevated risk categories contributing most to use.
Adherence to screening recommendations was not optimal, with screening advice arriving from multiple guidelines, public health messaging, and mammography result letters urging annual mammograms. Women screened more often than recommended, and increased magnetic resonance imaging use appeared among women assigned to elevated risk even though magnetic resonance imaging was not recommended for that category.
Researchers concluded that risk-based breast cancer screening that includes population-based genetic testing stratified risk and screening intensity without increasing stage ≥IIB breast cancers. Biopsy rates did not decrease, and observed screening behavior reduced separation between assigned strategies.
© 2025 Science X Network
More information Laura J. Esserman et al, Risk-Based vs Annual Breast Cancer Screening, JAMA (2025). DOI: 10.1001/jama.2025.24784 Nancy N. Baxter et al, Unlocking the Potential of Risk-Based Screening for Breast Cancer, JAMA (2025). DOI: 10.1001/jama.2025.24817 Journal information: Journal of the American Medical Association





Post comments